
Cryotherapy has been used to reduce chronic pain for many years due in part to its ease of use, affordability, and simplicity. It can be applied either locally (e.g., ice packs) or non-locally (e.g., partial and whole-body cryotherapy) depending on the location of the pain.
To determine the overall effectiveness of cryotherapy at reducing chronic pain by characterizing the currently available evidence supporting the use and effects of cryotherapy on chronic pain associated with chronic diseases.
A narrative review of original research studies assessing the efficacy of cryotherapy in alleviating chronic pain.
A PubMed database search was performed to find human studies between the years 2000 and 2020 that included the application of cryotherapy in patients with chronic pain associated with chronic diseases. A review of the relevant references was also performed to gather more articles. Data was extracted, summarized into tables, and qualitatively analyzed.
Twenty-five studies (22 randomized controlled trials, one prospective analysis, 1 one-group pretest/posttest study, and one case–control study) were included after the literature search. Both local and non-local cryotherapy applications show promise in reducing chronic pain associated with various chronic diseases including those of rheumatic and degenerative origin. Cryotherapy appears to be a safe therapy in carefully selected patients, with only minimal adverse effects reported in the literature.
Meta-analysis was not possible given the many differences between studies. Cross-study data homogenization and comparison between studies proved fairly difficult due to the lack of standardized studies, various uses and practice types of cryotherapy, and lack of control groups in some studies.
Local and non-local cryotherapy can be low-risk and easy treatment options to add in the management of chronic pain in carefully selected patients. However, long-term effects, a standardized approach, and careful study of other chronic pain syndromes should be considered in future research to further support the use of cryotherapy in the management of chronic pain.


Avoid common mistakes on your manuscript.
FormalPara Key Summary PointsThis is a review article discussing the uses of cryotherapy in treating different chronic pain conditions.
Local and non-local cryotherapy can be low-risk and easy treatment options to add in the management of chronic pain in carefully selected patients.
This article is published with digital features, including a summary slide, to facilitate understanding of the article. To view digital features for this article go to https://doi.org/10.6084/m9.figshare.13259225.
Cryotherapy is the superficial application of cold as a therapeutic agent. One of its most common uses is to alleviate chronic pain in specific areas through local application or more broadly through non-local application. Local application involves ice packs/bags, which can be specially designed or be as simple as waterproof plastic bags or frozen vegetable bags. Other local application methods include ice baths, ice massage, gel packs, chemical cold packs, vapocoolant sprays, or specialized cryocuffs that wrap around a joint and circulate cold water [1]. Non-local application of cold includes partial or whole-body cryotherapy. Partial-body cryotherapy excludes the head and neck, involves only one individual, and creates cold by spraying nitrogen gas directly onto the patient’s body. Whole-body cryotherapy (WBC) involves a large chamber fitting up to 3–4 patients, creating cold by either combining cooled nitrogen with oxygen and injecting it into the chamber or by circulating nitrogen within the chamber walls [2].
Cryotherapy has been around for ages, being noted in Aphorisms by Hippocrates as a pain reliever for both acute pain like hemorrhage or ankle sprains and its subsequent swelling and chronic pain such as chronic inflammation and joint pain [3]. Since then, physicians have strongly supported the use of cold therapy in alleviating chronic pain. In a 1697 letter to Prince William, Duke of Devonshire, physician John Floyer writes in full support of cold baths as a way to cure and reduce chronic pain associated with rickets and rheumatisms [4]. In an 1846 periodical, a physician wrote in on the benefits he found in his patients with cold water therapy, and one personal account notes the cure of their rheumatism and associated pain from cold therapy [5]. Physicians and physical therapists today still commonly prescribe cryotherapy as a way to reduce chronic aches and pains, especially due to the ease of use, simplicity, and low cost of this kind of therapy. However, while the use of cryotherapy in reducing chronic pain is very common, the exact mechanism and effectiveness still remains unknown.
In this paper, we aim to evaluate the effect of cryotherapy on chronic pain by reviewing the literature on both whole-body cryotherapy (WBC) and local cryotherapy (LC) on chronic pain caused by chronic diseases. We will first explain the proposed mechanism of action of cold therapy, then explain patient selection, and lastly explore the evidence and literature on benefits and adverse effects of cryotherapy.
An online literature search was performed using the PubMed database on the use of cryotherapy in chronic pain. The following terms were used to perform the search: cryotherapy, cold therapy, cold application, chronic pain, and pain. The search was limited to the English language, human studies, randomized controlled trials, clinical trials, and systematic reviews with results by year narrowed down from 2000 to 2020. A review of relevant references was also performed to gather additional articles. Studies focusing on acute trauma pain, post-operative pain, cryotherapy on healthy subjects (sometimes referred to as cryostimulation), and the use of cryoneurolysis or alternating heat and cold therapy were excluded, while those involving patients with chronic diseases that lead to chronic pain and/or had a detrimental effect on daily living were included. This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Although the mechanism of action of pain reduction by cryotherapy remains uncertain, there are a few primary theories that exist: reduction in inflammation/edema, oxidative stress, and nerve transmission in pain fibers.
Chronic inflammation can contribute to constant pain by chemical and mechanical stimulation of pain receptors and free nerve endings [6], which commonly occurs in autoimmune disease such as rheumatoid arthritis, ankylosing spondylitis, and multiple sclerosis. Thus, there is a strong interest in using cryotherapy to reduce inflammation in these chronic pain syndromes to hopefully also reduce the subsequent pain.
Edema and cytokines are key inflammatory markers used to assess the effects of treatments on inflammation. Edema is a cardinal sign of inflammation, caused by vascular changes and increased permeability that allows fluid to enter the extravascular space. The increased pressure in this space often leads to mechanical stimulation and pain production [6]. Cryotherapy is thought to decrease swelling [7] by a combination of decreasing vascular permeability [8] and reducing both arterial and soft tissue blood flow to the affected areas [9].
Cytokines are key regulators of the immune system that can work to maintain homeostasis, but also play an important role in driving inflammatory responses. In general, cytokines such as IL-1, TNF-α, IL-6, IL-12, and IL-17 are considered pro-inflammatory, while cytokine IL-10 is considered anti-inflammatory [10]. Studies have suggested that cryotherapy decreases inflammation by decreasing pro-inflammatory cytokine TNF-α [11,12,13], increasing anti-inflammatory cytokine IL-10 [14], and contrary to expectations, increasing pro-inflammatory cytokine IL-6 [11, 14,15,16]. However, new evidence suggests that IL-6 may also possess anti-inflammatory properties [17, 18]. In agreement, Straub et al. found an increase in IL-6 in patients with rheumatoid arthritis after WBC, with that group demonstrating the best clinical outcome as measured by swollen joint count and pain scores [16].
Another proposed mechanism of cryotherapy is reducing nerve transmission velocity in pain fibers [1], which may be a way that cryotherapy induces an analgesic effect and pain relief. Previous literature concluded that cryotherapy significantly reduced both motor and sensory nerve conduction velocity [19]. Algalfy and George found decreased nerve conduction velocity at the site of cryotherapy application, as well as increased pain threshold and tolerance. Of note, the effect on pain threshold and tolerance also extended distally to an area beyond the site of application, but supplied by the same nerve [20].
Oxidative stress has been associated with many human diseases including but not limited to cardiovascular diseases, neurodegenerative diseases, cancer, and rheumatoid arthritis. Oxidative stress can be a pathologic hallmark of autoimmune diseases, leading to more inflammation and adding to the constant pain a patient is in [21]. Studies have shown that cryotherapy may reduce oxidative stress by increasing total antioxidant status (TAS) [22, 23] and ferric reducing ability of plasma (FRAP), which is another way of measuring overall antioxidant status [24]. Additionally, research suggests that cryotherapy decreases total oxidant status (TOS) and oxidative status index (OSI), which is a ratio of TOS to TAS, as well [22, 24, 25].
As mentioned earlier, cryotherapy has been used to alleviate both acute and chronic pain. Acute pain is commonly associated with injury, infection, or disease, and is often easier to treat and relieve compared to chronic pain, which may not be associated with a physical injury. The most common mechanisms leading to chronic pain are mechanical or chemical irritation, nerve regeneration, motor reflexes, or inhibitory failure. Pain is usually considered to be chronic when it has persisted for longer than 3 months, lacks a correctable or identifiable cause, and medical treatments have not provided relief [6].
In this paper, the studies selected for the review involved chronic conditions that produced persistent pain. We divided the studies into three groups: rheumatic diseases, degenerative diseases, or a broad group of diseases under the name “other.” This was done because rheumatic diseases have underlying pathologies of dysregulated inflammation, whereas degenerative diseases have structural pathologies, which may or may not be accompanied with underlying inflammation. The rheumatic disease group consists of patients with psoriatic arthritis, rheumatoid arthritis (RA), gouty arthritis, and ankylosing spondylitis (AS), the degenerative disease group consists of patients with osteoarthritis (OA), chronic low back pain, adhesive capsulitis, musculoskeletal diseases, and myofascial pain syndrome, and the other group consisted of patients with chronic venous disease, fibromyalgia (FM), and multiple sclerosis (MS).
Cryotherapy is not safe for everyone and precautions must be taken. There is always a possibility of frost bite with exposures to very cold temperatures, especially with certain local cryotherapy applications such as ice massage or cold packs, that are left on for more than 20 min [1]. Whole-body cryotherapy also poses a risk of frost bite if precautions such as using gloves and hats and moving the fingers are not taken [2]. Another adverse effect is cold urticaria, which may have a small local reaction consisting of itching and red swellings to large, systemic effects such as facial flushing, hypotension, tachycardia, and syncope [6]. Cryotherapy is also contraindicated in patients with cryoglobulinemia, Raynaud’s disease, paroxysmal cold hemoglobinuria, peripheral vascular diseases, or insensate skin [1, 6, 26], so proper screening questions are essential prior to recommending cold therapy.
Chronic pain is a multidimensional experience, and it is important to focus not only on pain measurements, but also on range of motion and function in order to determine cryotherapy’s overall impact on chronic pain [27]. Chronic pain can limit range of motion and decrease function of the affected area by increasing pain with movement [6]. For this reason, the outcomes in this review will primarily focus on pain measurements, such as the Visual Analogue Scale for pain (VAS), with supplementary evidence including range of motion (ROM) and disease activity, such as Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Disease Activity Score 28 (DAS28) among a few others. For example, the BASDAI has six questions for patients with AS regarding fatigue, spinal and peripheral joint pain, peripheral swelling, tenderness, and morning stiffness [28] and the DAS28 includes parameters such as swollen and tender joint count, global visual analogue scale measuring overall patient health, and erythrocyte sedimentation rate [13, 29]. With these disease activity scores, a more generalized conclusion can be made as chronic pain can affect almost every aspect of a patient’s life.
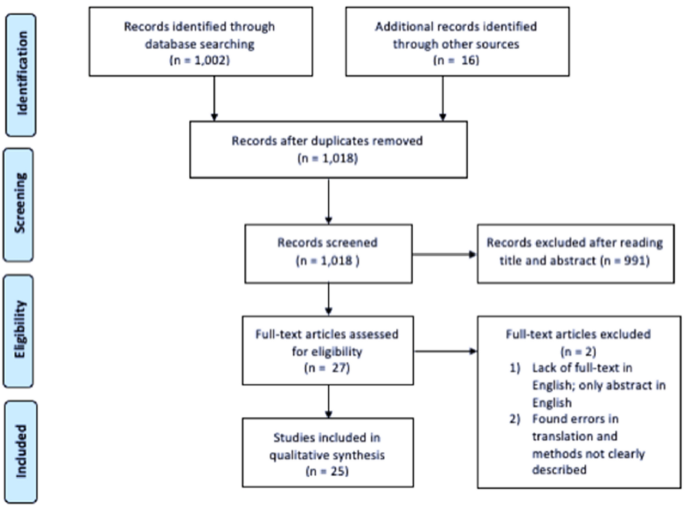
Figure 1 illustrates a flow diagram of the literature search and study selection, as adapted from Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRIMSA) [30], which lead to the 25 studies included in this review. The studies consisted of 22 randomized controlled trials, one prospective analysis, 1 one-group pretest/posttest study, and one case–control study.
Multiple studies have looked at the effect of cryotherapy on chronic pain caused by rheumatic diseases (Table 1). As mentioned earlier, chronic inflammation, which is present in chronic rheumatic conditions such as rheumatoid arthritis (RA) and ankylosing spondylitis (AS), can lead to persistent pain that often affects the joints [6]. WBC has been extensively studied in patients with AS. Stanek et al. reported in two different studies a significantly reduced mean pain (VAS) score following WBC at − 120 °C and rehab, along with a significantly greater reduction compared to the control group with just rehab [28, 31]. Stanek et al. also reported in two additional studies a significant decrease in disease activity as measured by BASDAI, and the WBC (− 120 °C) and rehab groups had a significantly greater reduction in BASDAI than the control groups that just received rehab [24, 32]. A decrease in BASDAI was also reported by Straburzynska-Lupa et al. in all their study groups (WBC at − 110 °C + rehab, WBC at − 60 °C + rehab, and control with just rehab), and it was noted that the group that underwent WBC at − 110 °C along with physical therapy had a greater reduction in BASDAI compared to the group that just received physical therapy. No differences after therapy were found between WBC at − 110 °C or − 60 °C [33].
Table 1 Rheumatic diseasesIn patients with RA that had undergone WBC, pain scores also seem to trend downwards, although there are contradicting findings. Both Gizińska et al. and Sadura-Sieklucka et al. found that WBC (− 110 °C and − 120 to − 140 °C, respectively) along with physical rehabilitation on patients with RA had a significant decrease in pain VAS, but results were not significantly different compared to the control group that only received physical rehab [12, 29]. Gizińska et al. also reported a decrease in disease activity (DAS28) and improvements in the 50-m walk test after WBC, showing increases in objective measurements of pain, but again those results were not significantly different than the control group. While these two studies suggest there is no additional benefit of adding cryotherapy to traditional rehab, it does not give insight into whether WBC as a standalone treatment would provide pain relief.
Straub et al. and Hirvonen et al. also looked at pain reduction in patients with RA after WBC at either − 110 °C or − 60 °C. Both studies found a significant decrease in pain (VAS) in the group that received WBC at − 110 °C, but not in the group receiving WBC at − 60 °C [16, 34]. However, the participants in the study by Hirvonen et al. also received physical rehab along with cryotherapy, but the study did not provide a control group that only received physical rehab. Additionally, a cross-over study in patients with inflammatory arthritis found that WBC produced a significantly greater reduction in pain (VAS) than the control group that did not receive WBC [35]. This study did not list the temperature of the WBC chamber, but the participants were instructed to stay 2 min in the chamber and the average skin temperature after WBC was 27 °C.
Local cryotherapy on patients with RA has also been investigated. Straub et al. found that LC did not provide any pain relief [16], but many others found significant improvements in pain following local application of cold [13, 34, 36]. One study that noted these improvements was conducted by Schlesinger et al., which required patients with RA to apply an ice pack for 20 min four times a day for a week. They found a significant decrease in pain (VAS) compared to the control group that did not receive LC [36]. In addition to pain relief (VAS) after LC, Jastrząbek et al. reported a significant increase in knee ROM along with improvements in the 50-m walk test in patients with RA, supporting the subjective measurement of decreased pain (VAS) [13]. Hirvonen et al. also noted a decrease in pain (VAS) along with a decrease in disease activity as measured by DAS in patients with RA who received LC [34].
Lastly, a significant decrease in pain (VAS) was also found in patients with gouty arthritis following application of an ice pack, showing a large reduction of 7.75 cm [35], further supporting the use of LC in treating chronic pain caused by rheumatic diseases. Based on the literature discussed, cryotherapy in the form of both WBC and LC seem to have positive effects on the chronic pain and clinical activity of the associated disease, with temperatures below − 110 °C showing the most benefit.
Cryotherapy has also shown promise as an additional tool in chronic pain management in patients with degenerative diseases (Table 2). One very common degenerative disease that often arises with aging is osteoarthritis (OA). WBC has not been a major focus in studies involving patients with OA, but LC has been explored in previous studies and shows promising results. Aciksoz et al. noted a significant reduction in pain (VAS) at rest, during movement, and during sleep after a 2-week course of cold pack application for 20 min twice a day and continued to see an improvement 2 weeks after the course was completed. Additionally, the Nottingham Health Profile was conducted to measure a patients self-reported social, physical, and mental health. The participants reported significant improvements in the subsections of physical mobility, emotional reactions, pain, and energy [37], suggesting cryotherapy not only has benefits for pain, but a patient’s overall quality of life as well.
Table 2 Degenerative diseasesAdditionally in patients with OA, ice application three times a week for 3 weeks also showed a significant decrease in pain (VAS) compared to pre-application pain scores, and had a significantly greater reduction than the groups that received short-wave diathermy (heat) or placebo [38]. Cold cryocuff therapy showed similar results, with 20 min twice daily applications for 5 days showing a significant reduction in pain (VAS and knee injury and osteoarthritis outcome score, KOOS) in those with OA compared to the control group that was directed to rest [39]. Dantas et al. reporting conflicting results in which ice pack application once a day for 20 min for 4 consecutive days did not show significantly different results than the placebo group that received an “ice pack” filled with sand, although both groups did show a decrease in pain (VAS) [40].
WBC, on the other hand, has been studied in other degenerative diseases including adhesive capsulitis, myofascial pain syndrome, musculoskeletal diseases, and chronic low back pain. WBC at both − 67 °C and − 5 °C reduced pain (VAS) and pain disability index in patients with chronic low back pain, and WBC at − 67 °C also reduced pain perception [41]. Similarly, Ma et al. reported a significant reduction in pain (VAS) after WBC at − 110 °C in patients with adhesive capsulitis of the shoulder, with a significantly greater reduction in the WBC and rehab group compared to the control group just receiving rehab. Additionally, there was an increased range of motion of the affected shoulder with a significantly greater increase in those who received WBC [42].
Moreover, García-Espinoza et al. found a decrease in pain (VAS) in patients with myofascial pain syndrome of the trapezius who received WBC at − 160 °C, along with an increase in pain tolerance [43]. Both LC and WBC seem to be beneficial options and should be considered in the management of chronic pain due to degenerative disease. Interestingly, WBC may have positive effects starting at higher temperatures in degenerative diseases (− 5 °C) compared to rheumatic diseases (− 110 °C).
Cryotherapy has also been explored as a method to alleviate chronic pain due to additional diseases such as chronic venous disease, fibromyalgia (FM), and multiple sclerosis (MS) (Table 3). It is difficult to draw a solidified conclusion on chronic venous disease and MS due to lack of studies in the literature. The one study we found on chronic venous disease, conducted by Kelechi et al., reported a reduction in both long-term (measured by Venous Insufficiency Epidemiological and Economic Study—Quality of Life/Symptoms, VEINES-QOL/Sym) and short-term pain (measured by the Numeric Rating Scale, NRS) in the group that received cryocuff therapy as well as the placebo group that received a cotton-filled cuff, with no significant differences between groups [44]. Since there were no differences between groups, it could be plausible that the compression from the cryocuff had an impact on pain rather than the cold therapy itself. In the one study on patients with MS, Miller et al. had the participants undergo WBC at − 110 °C to − 160 °C and noted an increase in motor function and decrease in disease activity [45]. Motor function was measured by the Rivermead Motor Assessment and looked at gross, leg and trunk, and arm function and disease activity was measured by both the Expanded Disability Status Scale and the Multiple Sclerosis Impact Scale. These give an insight into the objective effects of cryotherapy, however subjective, quantitative pain scores were not reported.
Table 3 OtherThere seems to be promising results for patients with FM. In patients with FM that received WBC, temperatures of − 196 °C, − 140 °C and − 110 °C were shown to benefit patient pain. Rivera et al. reported a significant decrease in pain (VAS) in patients with FM as compared to the control group after receiving WBC at − 196 °C [46]. Similarly, Bettoni et al. noted that patients that underwent WBC at − 140 °C had a significant reduction in pain (VAS). The control group also had a decrease in pain, but the group that received WBC had a significantly greater decrease in pain [47]. It was also found by Vitenet et al. that WBC at − 110 °C increased patients’ self-rated quality of life as measured by the Medical Outcomes Study Short Form-36, which includes questions about disease impact on function, daily living, mental health, and pain [48]. However, a stand-alone, quantitative pain score was not one of the outcomes measured.
Additionally, LC on patients with FM has also been noted by Yilmaz and Kiyak to be of benefit. They reported a decrease in pain (VAS) up to 24 h after cold pack application for 10 min [49], further supporting the beneficial effect on cryotherapy on pain reduction in patients with FM. More quality studies are required in order to draw a strong conclusion on whether cryotherapy offers benefit to patients with chronic venous disease or MS, but the literature supports that cryotherapy can be useful in the management of the persistent pain accompanying FM.
Cryotherapy seems to be a fairly safe therapy with only mild reports of adverse effects found in the included studies. Some of the adverse effects noted in patients that received LC include respiratory infection, frost bite, joint or muscle pain, and discomfort [34, 37]. Some of the adverse effects noted in those that underwent WBC include headache, hypertension, dizziness, malaise, joint or muscle pain, nervousness, respiratory infection, long lasting freezing, urticaria, slight aggravation of symptoms in the beginning days of treatment, a heartbeat feeling throughout the whole body, palpitations, sleep difficulties, bowel sounds and bloating, muscle stiffness, and tremor [28, 34, 46]. However, out of the 24 studies included, only four reported any adverse effects and most were short-lasting and mild. Careful selection of patients in the aforementioned studies likely limited complications.
Chronic pain is a crucial aspect in the management of many chronic diseases as it can have a profound effect on the function of the associated body parts and may significantly hinder a patient’s daily life. Cryotherapy has been around and used for the management of chronic pain for decades, dating back to the time of Hippocrates and still being commonly prescribed by physicians and physical therapists today. While such a common practice, the actual effectiveness of cryotherapy in reducing chronic pain has remained unknown. In this paper, we describe evidence for the effectiveness of cryotherapy in alleviating chronic pain due to a variety of chronic diseases.
The mechanism behind this pain reduction is thought to occur through the reduction of inflammation and edema, oxidative stress, and nerve conduction velocity in pain fibers. In regard to patients with rheumatic diseases such as gouty arthritis, psoriatic arthritis, rheumatoid arthritis, and ankylosing spondylitis, cryotherapy shows promising results. Whole-body cryotherapy demonstrated a reduction in both pain and disease activity, with temperatures of at least − 110 °C having the best results. Results also indicate that local cryotherapy can be an effective therapy in providing pain relief in patients with these diseases.
The literature on degenerative diseases including osteoarthritis, chronic low back pain, musculoskeletal diseases, myofascial pain syndrome, and adhesive capsulitis show similar results. In patients with osteoarthritis, results suggest benefits from local cryotherapy in relieving pain but evidence on whole-body cryotherapy is lacking. On the other hand, whole-body cryotherapy on other degenerative diseases show promising results, with results on pain reduction starting at temperatures of − 5 °C and continuing to temperatures of − 160 °C.
The studies included in the “Other” section included patients with chronic venous disease, fibromyalgia, and multiple sclerosis, and literature on these diseases was sparse other than fibromyalgia. The one study on chronic venous diseases found there was no effect of whole-body cryotherapy on pain, and the one study on multiple sclerosis suggested there was a pain reduction caused by whole-body cryotherapy, but the lack of studies on these two diseases make it hard to draw a solidified conclusion on cryotherapy’s effectiveness of these diseases. The studies on fibromyalgia, on the other hand, suggest that both local and whole-body cryotherapy provide pain relief.
It is important to note, however, that there are some limitations in our study. We found there to be a lack of standardized studies, with studies differing on temperature, duration of application, and study length. Additionally, there is significant variability in use and practice types. This made homogenization of data across studies in a meta-analysis impossible. Second, some studies lacked a control group, and often cryotherapy was used in combination with a standard treatment such as pain medications or kinesiotherapy. Again, this made cross-study comparison difficult and it is difficult to elucidate the precise role of cryotherapy amongst other standard treatments.
In general, we noticed that as long as patients are screened and those with prior conditions such as cryoglobulinemia, Raynaud’s disease, paroxysmal cold hemoglobinuria, peripheral vascular diseases, or insensate skin are advised not to use cryotherapy, cryotherapy is fairly safe with only mild and sparse side effects. Overall, evidence suggests that both non-local and local cryotherapy can be considered low-risk and easy treatment options to add in the management of chronic pain in carefully selected patients. Future research should focus on finding a more standardized application of cryotherapy, as well as include a wider array of chronic diseases associated with chronic pain. In addition, since chronic pain is persistent and long-lasting, future research should focus on the long-term effects of cryotherapy on chronic pain.
No funding or sponsorship was received for this study or publication of this article.
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Alaa Abd-Elsayed is a consultant for Medtronic, and Avanos. Carol Garcia, Jay Karri and Nicholas A. Zacharias have nothing to disclose.
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.